

LABOUR SUPPORT
This is a rough outline of the various skills we covered in our Clinical Skills Labour Support workshop.
Feel free to be in touch with any questions or clarifications! hello@ruthruttan.ca
OBJECTIVES
Our objective today is to raise awareness of our impact as humans on the labour and birth experience. We'll examine our presence, communication style, language, and actions and consider how we can be supportive in a birth space.
We'll use practical tools and role-play to explore how we can support the labouring person emotionally, physiologically, and anatomically.
An introduction!

photo by Creating Light Studio
Hi, I’m Ruth Ruttan. I'm a doula, prenatal & postpartum movement specialist and dancer. You can learn more about me here - Meet Ruth
My approach to supporting labour and birth involves several lenses: as an artist, I utilize connection and creativity; as a movement expert, I draw on anatomical knowledge and an understanding of movement and instruction; and as a doula, I leverage my training to support physiological processes.
Obviously, doulas come in all forms and labour support can look many ways! I'm hoping that as you support births, you can draw on your unique skills to form your comfort in the birth spaces.
I'm also hoping that by the end of our time together, whether you're experienced in the birth world or not, you'll have some tools for entering a birth space, bringing calm and comfort, feeling at ease, and connecting with your clients' natural rhythm.
It would be absurd to think we could cover everything related to support, so I've selected a few key areas for us to focus on.
Environmental and emotional support.
Communication and language.
Physical support for common discomforts and labour scenarios.
Let's make some assumptions—we are looking to support what's happening physiologically and anatomically, while also addressing emotional and comfort needs. Even if a birth isn't purely physiological, we can still encourage it in this manner.
You'll have limitations imposed on you by the expectations and other responsibilities given to you by your preceptor. Sometimes, you will only be able to utilize a few of the tools you’ll learn, but you can keep these in your back pocket for when an opportunity arises.
Breathwork
Before we begin, let’s do some calming breathing together. Find a relaxed position, either seated or standing, with your hands on your forehead, heart, or belly. Eyes open or closed, breathe in through your nose for 4 counts, out through your mouth for 6 counts. (This is just one form of calm breathing; there are many)
Soften your face, soften your jaw, and drop your shoulders. Sink into the surface you're sitting on and let it hold you. (these are great phrases to say to a labouring person, too!)

Ruth Ruttan is applying sacral counter-presser on a client at the Toronto Birth Centre while a student midwife holds their hand, and a midwife observes. Photo by Heather Bays Photography.
Debriefing our Roleplay
A brief discussion on the environment and the scene that was unfolding as you walked int the room.
I will aim to add a list of observations and thoughts from each group after our workshop day. Below is a list of items we developed last year.
Environmental & emotional support.
Some practical suggestions you can riff off of when you walk into a birth space:
• Before you enter, take a few breaths to centre yourself and become present to 'what is'
• Check your fears, biases and expectations at the door.
• Notice the environment and what's in it.
• Who's in it? Introduce yourself to support people, including the doula!! And what role do you have?
• Between surges, introduce yourself to the birther and what role you're in. Example: I'm a student midwife. I'm here to support you and your family, both emotionally and physically, if needed, and to assist your midwives.
• Check in on the support people - do they need to hydrate, eat, rest, be reassured?
• Check in on the labouring person. Do they seem to be coping well? Offer them water or snack.
• Is there anything in the environment that could change to support physiological birth? Check the five senses and help fill them with calming elements.
• Ask questions of the support people to get a sense of why the room is as it is. If you want to change something, ask the support people and the labourer.
• Find out about their language & birth preferences:
Examples: Contractions vs. Surges, tightenings, waves or Pain vs intensity, what is your comfort level vs. how much pain are you in.
• If you have the opportunity, stick by the doula and see what skills they are using. They typically have an existing relationship with the family and an understanding of their birth preferences. You'll either bond over being newbies or learn from each other.
PHYSICAL SUPPORT

Ruth Ruttan is doing some downward strokes on the shoulders and arms of a client at the Toronto Birth Centre. Photo by Heather Bays Photography.
These are to help a labouring person find their natural rhythm or flow & show that you are trustworthy!
What sounds are they making - deep guttural/high-pitched, screaming? Model the type of breath you want them to do - Slower, deeper sounds - video of a beautiful birther vocalizing in their labour
Let's play detective!!
Ask to touch the labouring person’s back and sacrum - this may be able to help you assess the station of the baby or if there's a misalignment without doing a vaginal check (but this can take practice and doen’t work with everyone!)
Notice tension in their body? Scrunched face? Clenched hands? Shoulders up?
You may ask where they're feeling surges or discomfort/ pressure? Belly, hip(s), back, a combination of those?
What sounds are they making - deep guttural/high-pitched, screaming? Mimic the type of breath you want them to do - Slower, deeper sounds - video of a beautiful birther vocalizing in their labour
Is there bloody show?
Get a sense of the labour pattern if you can (ideally from a support person or time a few yourself)
These questions may give you an idea of what physical tools might feel best.
Supportive Touch:
BUTT BREATHING: down-regulates the nervous system, releases tension in the body, mobilizes the sacrum, creating better balance in the body and torso - anatomically promotes more space for the physiology
HOW: All fours (over a birth ball), one hand on sacrum (fingers point to head), one hand on ribs (fingers point to head).
Inhale gentle traction apart - sacral counter nutation (tuck under)
Exhale, hands gently come together - sacral nutation (extends out)
WHEN: to address fear, help with mindset, provides a nice introduction to working together, prodromal labour, malposition, and imbalance in the labouring person's body. It can be used in so many scenarios!
I’ll try to upload a video of us doing this in the next few days!
OTHER TOUCH:
• Stroking down the legs, holding ankles, heat on lower/ upper back, holding ankles or feet, stroking shoulders or shoulders down to arms - watch video here
• Shake the Apple Tree - watch a video here

Ruth Ruttan is doing the double hip squeeze on a client at the Toronto Birth Centre. Photo by Heather Bays Photography.
• Counter pressure - sacral, pressure points in the dimple of cheeks, knees - add shifting
• Double Hip Squeeze (see picture!)
Communicating & Language:
Your communication style and language play a significant role in supporting others.
• Tone & Volume - lower your voice in tone and volume, speak between surges, limit questions to consent, keep options concise - don't offer a laundry list.
Be encouraging.
• Support their decision-making:
Ask if they feel they have enough information or offer to explain in layperson's terms.
Protect the labouring person by offering time to discuss without watching eyes.
Examples of things to avoid:
• Now I'm going to... I'm going to do this... ALWAYS ask for consent!
• Bad babies, misbehaving babies, gender stereotypes - “they're so stubborn and won't turn for me - must be a boy.”
Click here for A story about language.
Supporting Anatomically
Let’s investigate how the movement of our body impacts the movement of the pelvis:
With your hand(s) on your ASIS, move your legs in various directions.
With your hand on your tailbone/ sacrum, move your legs in various directions. Try raising your arms overhead.
Try these movements in various positions: all fours, supine, sidling, and standing, and see what you notice about your pelvis. You should feel movement!
Anatomical Reminders!!
To open the top of the pelvis (inlet): external leg rotation (knees wide apart) and hip extension (front of the hip open)
To maneuver through the mid pelvis - a combination of hip extension and hip flexion.
To open the lower pelvis (outlet): deep hip flexion (bent at the hip), internal leg rotation (but the knees DO NOT need to be close together!), arms reaching can also help free the sacrum (tailbone).
Movement for Baby’s Station
Baby is “floating” high in the pelvis or early labour - to encourage engagement:
• Assess sacrum if possible
Restful positions:
• Flying Cowgirl
• Lift & Tuck
• Walchers/ hip extension
• Penny Simkin’s Roll Over Method:
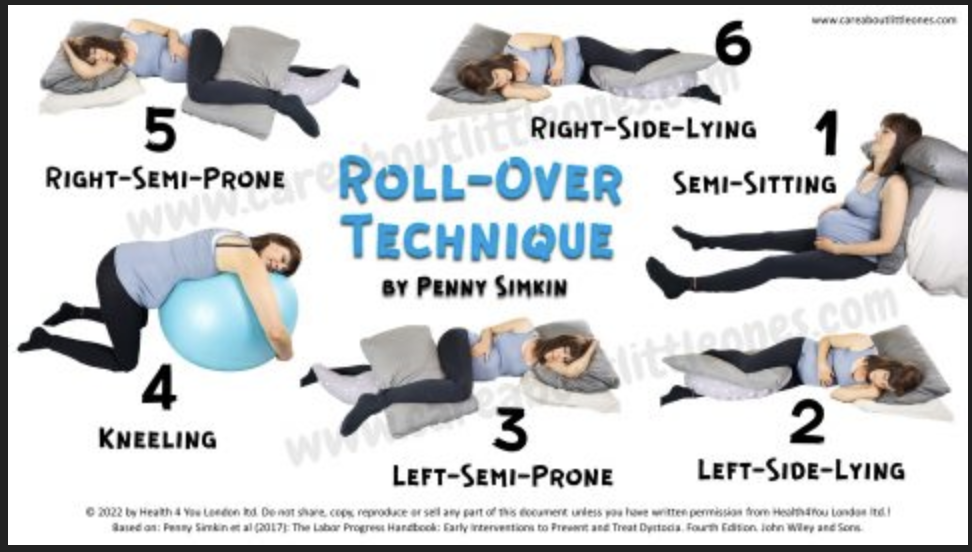
This technique is a series of positions designed to help promote labour progress, especially when the birthing person is confined to bed, for example, due to an epidural. The image shows six different positions:
Semi-Sitting
Left-Side-Lying
Left-Semi-Prone
Kneeling
Right-Semi-Prone
Right-Side-Lying
These positions are typically used in a sequence, often with a peanut ball for support in some of the positions, to encourage the baby to descend and rotate in the pelvis.
Twice through if possible.'
Movement & Active positions:
• Cat/Cow
• Birth ball hip movements - watch video here
• Leaning squats & side lunges - watch video here
Baby is in the Mid Pelvis:
ROCK THROUGH THEORY: All movement is good and can help the baby navigate the pelvis - explore alternating movement.
Passive:
• If there is an epidural, you move their leg, rocking in positions with a peanut ball
• Roll Over Method - Penny Simkin. see above.
Movement & Active positions:
Asymetric movement: Slow dancing w/ one leg elevated, lunging w/ one leg elevated, Kneeling aligned lunges (psoas stretch is a bonus), curb walking or stair stepping, standing psoas release, Dip the Hip, Glute Scoot. - video of some partner supported movement
All fours & Kneeling lunges
Lots of examples of all of the above in this video!
Pelvic Outlet & Second Stage:
Before a birther starts actively “pushing,” there may be an opportunity for Passive Decent (letting the surges/ contractions bring baby down lower in the pelvis before they start pushing) Here’s a video of using the toilet to Labour Down (passive decent) - watch video here
Various Positions for opening the pelvic outlet and pushing:
Typically positions with deep hip flexion, internal rotation of the femur (knees do not need to be together!) and often with the arms in flexion - reaching or pulling (the latissimus dorsi connects to the sacrum and nutates the sacrum when arms are in flexion) - check these out
Side, All fours, seated or standing squat, hanging squat, kneeling, standing one leg elevated, back with a runway.
• We DO NOT push with our legs or our pelvic floor!
Many midwifery client want to “breathe their baby out” rather than directive pushing. Directive pushing is what is most commonly use by all types of healthcare providers. This is an interesting topic that you can have conversations about and digest over time.
SPECIAL CIRCUMSTANCES:
Prodromal labour/start-stop labour:
Labour is intense and frequent, but progress is (relatively) slow
Address their mindset & create balance in the body/ pelvis
Butt breathing
Standing Psoas Release
Aligned kneeling stretch with overhead arm/ Flying Cowgirl
Walchers Stretch
OP/ OT/ malpositioned baby, Baby needs to Rotate:
Possibly an inversion off a sofa or on a hospital bed with the leg portion lowered (elbos on the lowered part), open knees and chest, or supported hips up in bridge.
Sacral rocking/ release -all fours, side lying, standing
Side Lying Release (3 surges on each side) do not do with clients with SPD
Extreme side lying with rocking
Baby may be Asynclitic:
Asymmetry in the sacrum could indicate that baby is asynclitic or maybe their arm is up and in the way, the head compounded somehow
Chiropractor - can one come to the birth location?
Inversion - actual inversion or open knees to chest/ bridge
Sacral rocking/ release - all fours, side lying, standing
Asymmetrical Seated Thrown
Thank you for attending this workshop!

Photo of Ruth Ruttan doing counter pressure on a clients hip while they squeeze Ruth’s wrist. Photo by Heather Bays Photography.

Let’s chat!

Be in Touch
I take on a limited number of births and postpartum families each month so as to be able to fully support each family. It’s never too early (or too late!) to get in touch - no question is too big or too small! I am always happy to chat about anything related to your pregnancy to parenthood journey.
What People Are Saying
“Ruth is truly a remarkable human being and an invaluable doula. You need to hire her - you will not find anyone comparable.”
I am not sure where to begin. Ruth is truly a remarkable human being and an invaluable doula. You need to hire her - you will not find anyone comparable. She is so knowledgable, present, caring, intelligent, and supportive. She will advocate and help you at every step of your process. She communicates clearly, provides endless resources, and is available when you need her. There are no silly questions with Ruth - she will help you be informed about your options and realistic about best routes. She will talk to your doctors or midwives if you do not have the energy or capacity to do so to ensure your desires are communicated. During labour, Ruth was remarkable. She helped me achieve my most ideal birth at home with midwives and was amazing at helping me work through waves of pain.
I know she would have been just as supportive and helpful in a hospital setting with an epidural, or with a belly birth. She is just the kind of person who is always there for you. I cannot recommend her enough. We hired her early on in our process and would do the same again because it was so helpful having her when things were hard in our second trimester. We really got to grow together and learn together. Thank you for everything Ruth! We hope we can have you on our team again in future pregnancies!!
— Laine, Joanna & baby Ty